Introduction
As we near the end of the first decade of the 21st Century, the pace of change in healthcare is accelerating, spurred on by faster and faster IT advances. The challenge is now to keep up with the pace of technology change rather than, as in the last century, conforming technology to the existing healthcare paradigm. Everybody agrees that the patient or consumer-the individual person-must become the focus of the new model of care, whether from a chronic disease, customer service or patient-flow perspective. What's needed now is a new intellectual framework for achieving this objective in a technology-rich universe. Enter the Data Corridor.
The Data Corridor is a four-stage evolutionary path for a healthcare organization to move to a future state of data maturity by the year 2015. It replaces the old, static concept of building a layered IT infrastructure with a new, dynamic and forward-looking framework better suited to the promise of the 21st century. A significant differentiator for the Data Corridor is that it captures patient-centric information from an operational perspective-seeing healthcare as a human supply chain-rather than from a clinical one. This important shift allows healthcare organizations to apply industrial metrics where they can be most effective and allows them to become high performance organizations.
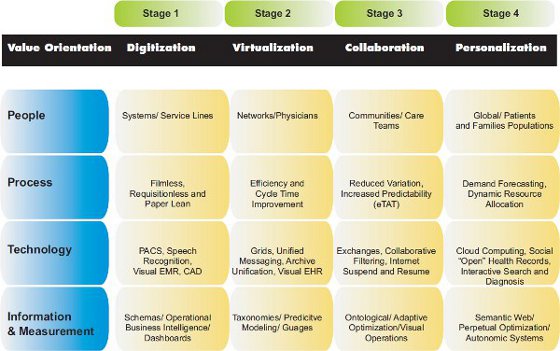
The Data Corridor is based on four layers: People, Process, Technology and Information, and Measurement. There are four stages that mark the journey through these corridors: Digitization, Virtualization, Collaboration and Personalization. The key element that makes this journey of maturation successful is Data Certainty, the factor that ensures data integrity endures from the first stage to the final one. The closer you get to maturity, the more certain you need to be of the data.
Stage 1: Digitization
Technology is the driver at this stage, which is where most organizations are today. Physicians need the best technology and therefore hospitals want to market the best technology to recruit the best doctors. Even at health systems with relatively low levels of digitization it's possible for patients to have digital images acquired and archived, most bedsides have telemetry systems and the beds themselves are "online." Departments like laboratory, pharmacy and others have been going digital for a long time. Hospitals acquire technology to achieve quality of care standards, support patient safety initiatives and capture digital evidence to develop repositories and archives required for advanced clinical systems such as CPOE and clinical decision support (CDS).
Big idea on data:
Capture it digitally at the head of the line, capture it once, expose it in real-time
to those on the front lines who are delivering service.
Current systems are designed to feed the macro systems and their associated missions such as being the best in cancer care, pediatrics or women's health. CMOs and clinical chairs focus on clinical quality and development of Centers of Clinical Excellence that are closely aligned with the organization's mission and brand. The Digitization Stage can provide IT-enabled advantages like reduced film and paper through a PACS, which enables centralization and distribution of medical images across standards-based platforms.
Stage 2: Virtualization
In this stage, technology is used to allow care teams to access systems from anywhere using secure mobility. IT's foundation elements now go beyond a one-to-many utility to that of a many-to-many grid. An everyday example: Just about anyone can log into email from anywhere using one of multiple devices and displays.
Big idea on data:
Formats and standards will evolve and change - your data must endure.
The lowest common denominator of a device allows a person to read a message. You can't achieve this kind of capability in healthcare unless you're certain about the quality of your data, and that begins with an initial inspection and cleansing, followed by continuous profiling of data during transactions. With Virtualization the ability to generate operational data is key. The value of virtualization is to pool resources, match skill to demand and eventually to match supply to demand. Digital systems can trigger alerts when:
- an order is placed
- someone logs in
- a nurse "punches in"
- a patient is moved
- a bed is available
There are many patient hand offs, and many resources involved in the human supply chain - to be able to harmonize these operational triggers - from the standpoint of the resources providing the care.
Stage 3: Collaboration
This stage is characterized by organizational analytics in which the exchange of data is designed so frontline staff-those who work with patients, families and physicians-can glean insight from operational data streams to achieve business agility and adaptive business intelligence. Processes are digitized and mined for perpetual analysis of variance, which yields increased predictability for resource planning and human-resource allocation. Also, in terms of both the patient and physician experience, estimated Turn-Around-Times (eTATs) and other cycle times can be defined to proactively manage expectations. To organize data into ontologies is an aggressive task that occurs around clinical service areas and those areas benefit from evidence sharing to further the development of collaborative visual search systems and distributed computer assisted decision support.
Big idea on data:
Data is valuable, but only if it's precise, accurate and clean. You must be certain of your data.
Just as clinical grid systems like CaBIGTM emerged in a wave of clinical knowledge transfer, financial and operational benchmarking grids will emerge to support AHRQ metrics related to satisfaction.
Stage 4: Personalization
If there's a single theme to this stage it is social media. In healthcare terms that can mean the online matching of people with specific diseases, conditions or needs with individuals or support groups who can help them. Essentially, it involves using online collaboration to match supply and demand. In that sense, the Personalization stage defines healthcare in the broad context of the global community of professional and nonprofessional caregivers, including chronically ill people who have become experts at managing their own diseases, parents of ill children and other self-developed experts. Everyone will eventually "root" somewhere electronically-you might call it an eMedical Home- whether it's GoogleTM with a unique identifier, MicrosoftTM HealthVault or another form of online PHR.
Big idea on data:
Naming convention, the meta/resource layer of data is critical. You need common descriptors to support virtualization.
In this stage, data quality becomes more valuable than ever. Data will be structured around personal coaching and enhancing the patient and family experience using communities and support tools; data mining will become a tool for identifying and targeting large global populations and for demand forecasting and dynamic resource allocation. Interactive search and diagnosis will become standardized.
Summary
The 2015 Data Corridor provides a framework for leveraging the lightning pace of technology change in 21st Century healthcare while ensuring data integrity every step of the way. The four stages of Digitization, Virtualization, Collaboration, and Personalization integrate the five corridors of people, process, technology and information, and measurement to provide an operations-based path into the future. To achieve usable data, to capitalize on the Digitization, Virtualization, Collaboration and Personalization of medicine, it must be clean, accurate and precise. What better time than during the migration of systems to bring data to a pristine state.